
Olfactory nerve
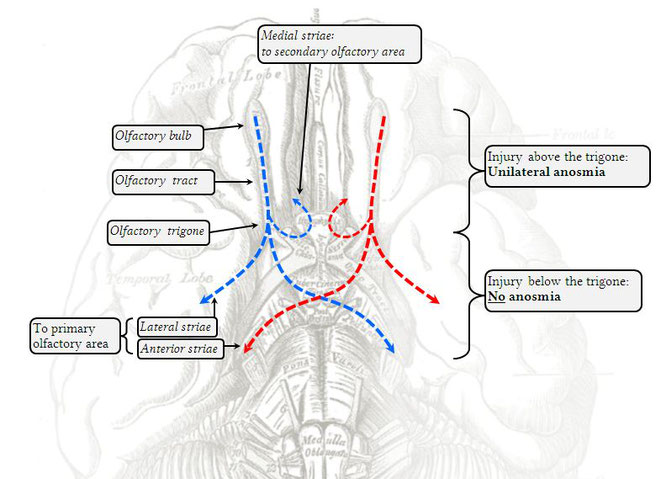
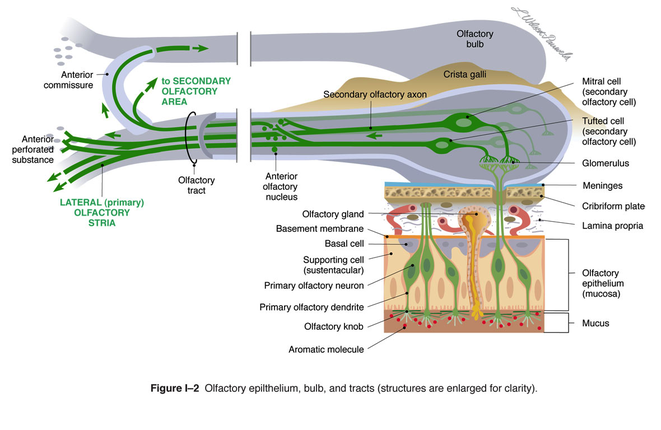
The olfactory nerve, around the area of the optic chiasm, divides into three striae (trigone). These are the anterior, medial and lateral striae. The lateral striae travels to the ipsilateral olfactory cortex in the uncus, and the anterior stria cross the anterior commissure to communicate with the contralateral olfactory cortex. Additionally, it appears the olfactory bulbs talk to each other via the medial striae, and a fair amount of neural processing seems to occur in the bulbs themselves.
The olfactory bulb is said to receive its blood supply from the branches of the anterior cerebral artery, whereas the primary olfactory cortices are irrigated by the lenticulostriate arteries arising from the first segment of the MCA, by the posterior temporal branches of the MCA, and possibly others. The areas of the brain involved in olfaction are actually quite widespread, which makes it difficult to use it in infarct localisation.
Generally speaking, an isolated unilateral stroke in the primary olfactory area will not yield any clinically significant olfactory symptoms - the contralateral area should still receive bilateral olfactory information. However, case reports demonstrate that the olfactory cortex shares some vascular real estate with the gustatory cortex, and abnormalities of taste perception may develop with isolated strokes of the insula.
Examining the olfactory nerve:
Bilateral anosmia: neither nostril can smell anything.
Unilateral anosmia: one nostril is affected.
Hypoosmia: the sense of smell is present but its sensitivity is decreased.
Hyperosmia: the perception of smells is pathologically exaggerated.
Dysosmia: the sense of smell works, but is distorted.
Olfactory hallucinations: sense of smell without the odour being present.
Causes of bilateral anosmia
Both nostrils damaged or blocked
- Trauma
- Tumour
- Sinusitis/rhinitis
Both cribriform plates or olfactory bulbs are destroyed
- Trauma
- Tumour
- Meningitis
Congenital olfactory bulb dysfunction
- eg Kallmann's Syndrome
Cellular sensory apparatus insensitive
- Smoking
- Chemotherapy
- Radiotherapy
Causes of unilateral anosmia
Nostrils damaged or blocked, cribiform plate or olfactory bulb destroyed
- Trauma
- Tumour (specifically: olfactory groove meningioma
- Sinusitis/rhinitis
Causes of hyposmia
- Smoking
- Nasal polyps
- Chemotherapy
- Chronic industrial solvent exposure
- Vitamin A deficiency
- Pernicious anaemia
- NIDDM
Causes of hyperosmia
- Addison's disease
- Cystic fibrosis
- Pituitary tumours
Causes of dysosmia
- Alzheimer's disease
- Korsakoff's Syndrome
- Parkinson's disease
- Huntington's chorea
Causes of olfactory hallucinations
- Migraine
- Schizophrenia
- Temporal lobe epilepsy