
Musculocutaneous nerve
The musculocutaneous nerve arises from the lateral cord of the brachial plexus, and therefore contains fibres from spinal roots C5, C6 and C7.
After originating from the brachial plexus, the musculocutaneous nerve leaves the axilla, and pierces the coracobrachialis muscle, near its point of insertion on the humerus.
It then passes down the arm, anterior to the brachialis muscle but deep to the biceps brachii, innervating them both. The nerve emerges laterally to the biceps tendon, and continues into the forearm as the lateral cutaneous nerve. It provides sensory innervation to the lateral aspect of the forearm
The musculocutaneous nerve is well recognised to have a varied anatomical course. It can interact with the median nerve, adhering to the nerve and exchanging
fibres.

Click image to enlarge
Motor function
The musculocutaneous nerve innervates the muscles in the anterior compartment of the arm – the biceps brachii, brachialis and coracobrachialis. These muscles flex the upper arm at the shoulder and the elbow. In addition, the biceps brachii also performs supination of the forearm.
Sensory function
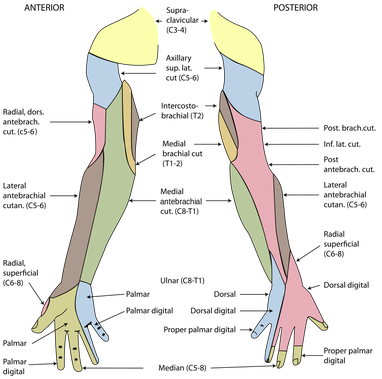
The musculocutaneous nerve gives rise to the lateral cutaneous nerve of forearm.
This nerve initially enters the deep forearm, but then pierces the deep fascia to become subcutaneous. In this region, it can be found in close proximity to the cephalic vein.
The lateral cutaneous nerve of forearm innervates the skin of the lateral aspect of the forearm.
Click image to enlarge
Clinical relevance
The arrangements of the fibrous sheaths of the corocobrachialis muscle allow for a 'telescoping' effect in relation to the musculocutaneous nerve. Any factor which decreases this sliding effect may expose the nerve to mechanical effects of muscle contraction, with the possibility of a compression syndrome.
Lesions of the nerve produce weakness of flexion at the elbow and weakness of supination. The biceps is an important supinator. There is sensory loss on the lateral side of the forearm. The brachialis muscle receives innervation from both the musculocutaneous nerve and the radial nerve. One study found that the musculocutaneous nerve contributes to 42% of the muscle power that flexes the elbow.
Isolated injury to the musculocutaneous nerve or the lateral antebrachial cutaneous nerve is rare.
Risk factors
- Damage to the shoulder and brachial plexus can affect the musculocutaneous nerve.
- Compression of the nerve by the biceps aponeurosis and tendon against the fascia of the brachialis muscle causes sensory loss below the elbow on the lateral side of the forearm. Entrapment of the nerve is one cause of pain at the elbow.
- During shoulder joint replacement, before placing a retractor on the medial side of the incision to retract the conjoined muscles and pectoralis major, it is necessary to palpate and identify the nerve to avoid damage.
- Using an anterolateral approach to the humerus during orthopaedic surgery also carries a risk.
Clinical signs
The following features are characteristic:
- Weakness of elbow flexion and forearm supination.
- Sensory loss over the lateral and volar aspect of the forearm.
- Weak or absent biceps tendon reflex.
- Being a lower motor neurone lesion, other expected signs include poor muscle tone, marked wasting and possibly fasciculation