Tumor mimics - infections
There are multiple infections that may mimic intracranial tumors. Aside from cerebral abscesses, two distinct forms of tumor mimics are tuberculoma and neurocysticercosis. The radiographic features of cerebral abscesses in general are discussed elsewhere on this website.
Tuberculoma
Tuberculoma is one of the intracranial manifestations of tuberculosis, along with tuberculous meningitis and tuberculous abscesses. The distinction between a tuberculoma and tubercolous abscess is the the presence of granulomatous reaction and caseous necrosis. Tuberculous abscesses do not have a granulomatous reaction and their centres are filled with pus. MRI is the modality of choice in assessing potential tuberculomas which have fairly solid caseous necrosis centrally on the background of granulomatous reaction. In some instances, liquefactive necrosis centrally may occur, making the lesions virtually indistinguishable from tuberculous abscesses.
MRI features
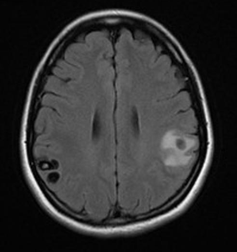
T1: T1 imaging shows isointense signal compared to grey matter and lesions may have central region of hyperintensity representing caseation.
T2: On T2 weighted imaging lesions are isointense to grey matter but may have central region of hypointensity representing gliosis and abundant monocyte infiltration. Lesions are surrounded by vasogenic oedema.
T1 C+ (Gd): Contrast series usually show ring-enhancement and lesions may appear as a conglomerate enhancing mass.
DWI: Usually there is no diffusion restriction. When liquid necrosis is present there may be a high central signal.


Neurocysticercosis
Neurocysticercosis (NCC) is a CNS infection caused by the pork tapeworm Taenia solium, which is endemic in most low-income countries where pigs are raised. It is a relevant cause of seizures in endemic areas. The disease may be located intra- and extra-axial. Common locations are the subarachnoid space, the parenchyma of the brain (usually near the grey matter-white matter junction), or the basal cisterns and 4th ventricle.
The appearance of lesions may be 'grape like' (racemose) and most lack an identifiable scolex. Intraparenchymal cysts tend to be small (1cm), where intraventricular lesions may grow up to 9cm.
Epidemiology
The disease is endemic in Central and South America, Asia and Africa. The perpetuation of this parasitic disease is related to poor sanitation and hygiene.
MRI features
MRI imaging can be variable depending on disease stage. In general lesions may show high signal on T1 weighted imaging compared to grey matter and the hyperintense scolex on T1 can sometimes be seen. Surrounding oedema may be present and ring enhancement is present as of the colloidal vesicular stage of the disease.